Jan 12, 2023
This past May, the University of Texas at Dallas announced the groundbreaking for the new Crow Museum of Asian Art…

Smudged mirrors. Trashed bathrooms. Filthy hands. Humiliating encounters. These are the experiences people with vision impairments describe of feeling — quite literally — their way around unfamiliar bathrooms, attempting to find and operate the soap dispenser, towels, faucets, hand dryers, and so on. They must ask strangers for help washing and drying their hands — a practice critical to preventing pathogen spread. When no one is there to assist, they may leave less clean than when they started muddling around a strange restroom in darkness. These testimonies represent one of the ways that the design, elements, and use of a facility influence pathogen spread. These stories expose the inexcusable inequity and heightened risk of serious infection within the disability community.
Responses in architectural design to the current pandemic are naturally lagging behind medical sciences; vaccines and therapeutics take priority. However, this does not obviate the design industry’s potential for impact at this historic moment. The architecture industry has an imperative to look for solutions to reducing the spread of SARS CoV-2 and future pathogens for everyone.
Pandemic Hardening and Panic/Neglect Cycles
Pandemic hardening in the design and operation of a facility is a concept for diminishing discrimination toward persons with disabilities (PWD) by proactively reducing pathogen exposure and spread. Discrimination for PWD is occurring in the form of an inherently increased risk of contact with pathogens, compared to the overall population.
With each epidemic or disaster, society engages in a cycle of panic and neglect. In 2020, during the early stages of the pandemic, the public cleared the shelves in panic-buying of hand sanitizer, toilet paper, food, and medicines. But as disasters wear on over time, people often return to habits and behaviors to which they were previously accustomed, as is the case with mask fatigue. The industry of architecture cannot justify forgetfulness or negligence. The opportunities for advancing the health, safety, and welfare (HSW) of all building users must be embraced — and more so for the most vulnerable.
“Post-Pandemic”
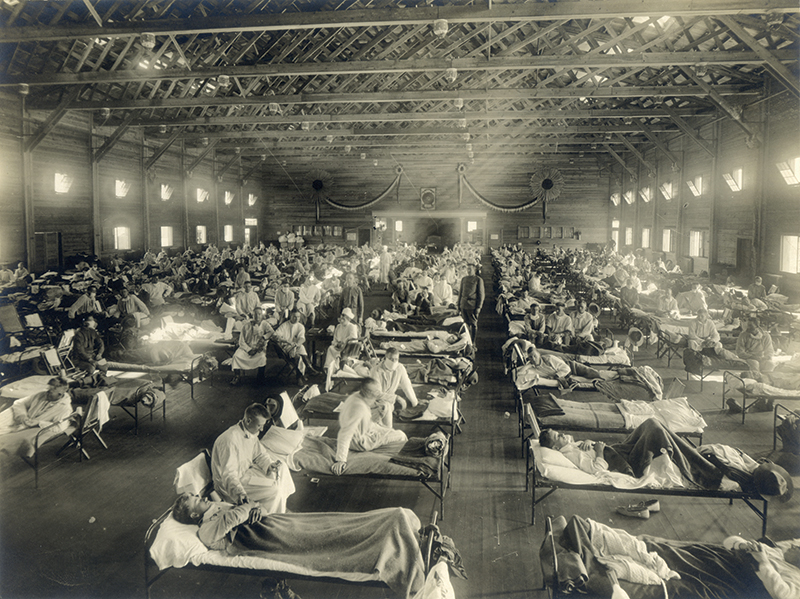
The concept of a “post-pandemic” era is a fallacy. Humans have dealt with plagues throughout recorded history, from the bubonic plague that left more than 50 million dead, to the Spanish influenza of 1918, to this current pandemic, among others. The architectural industry has historically been unable to offer sweeping, effective solutions to the many plagues that have ravaged our globe. The current technologies, products, materials, and advances in medical science simply were not available, necessary, or effective. HIV/AIDS is one recent example of a pandemic where there simply are no beneficial architectural strategies.
Doctors treated tuberculosis (TB) and the Spanish flu with quarantines, fresh air, and sunlight. The 1918 influenza is one of the early examples in which building design had a reactive role in treatment, resulting in a national movement to increase fresh air via fenestrations. One lackluster response was the development of radiator heating systems to compensate for open windows in winter.
In the 1940s, TB clinics, in collaboration with designers and scientists, began compartmentalization of patient rooms. As HVAC technologies advanced, designers began segregating airflow and increasing fresh air ratios, and these same methods are proving invaluable now.
In 1976, Legionnaires’ Disease revealed how water vapor and plumbing systems exacerbate disease spread. Similarly, a 2021 study of a high-rise, multifamily structure in Guangzhou, China, suggests that CoV-2 spread via the plumbing vent system and/or the force of flush toilets, including one confirmed case on a single floor that caused the building to be vacated. Regardless, the virus spread to empty, adjoining floors 12–15 stories above.
Codes and Standards
The building codes and Americans with Disabilities Act (ADA) Standards for Accessible Design represent advancements for PWD, and the provisions continually evolve after disasters. But they are design minimums, with no pandemic modeling standards informed by this ongoing disaster. No enforceable, substantive architectural revisions have been developed in response to this pandemic yet — nor have any adjustments been made looking ahead to the next one, which will inevitably come.
Federal organizations and private industries endeavor to keep pace with medical sciences in this pandemic. The ADA National Network (ADANN) is collaborating with the International Code Council (ICC), the American Institute of Architects, the Texas Society of Architects’ Equity, Diversity, and Inclusion Committee, and other state and national agencies to develop a more concerted response. The AIA produced multiple “Reopening America” publications with strategies for existing buildings as this scourge swept the world. Their dedication is also evident in their HSW programs. Pandemic hardening is a model that aligns well with the HSW classifications as well as many LEED categories, including Innovation, Indoor Air Quality, Volatile Organic Compounds Control, and others.
Disability Types and Increased Risks
Chair Users
According to the Centers for Disease Control, 61 million Americans have some type of disability. Mobility impairments represent about 70 percent of that total. But that ratio by no means diminishes the needs of others with different types of physical and mental impairments. A wheelchair is just one accommodation to mobility impairments. (In our industry, we avoid saying wheelchair-bound or handicapped.) Canes, walkers, heart conditions, and asthma also affect mobility.
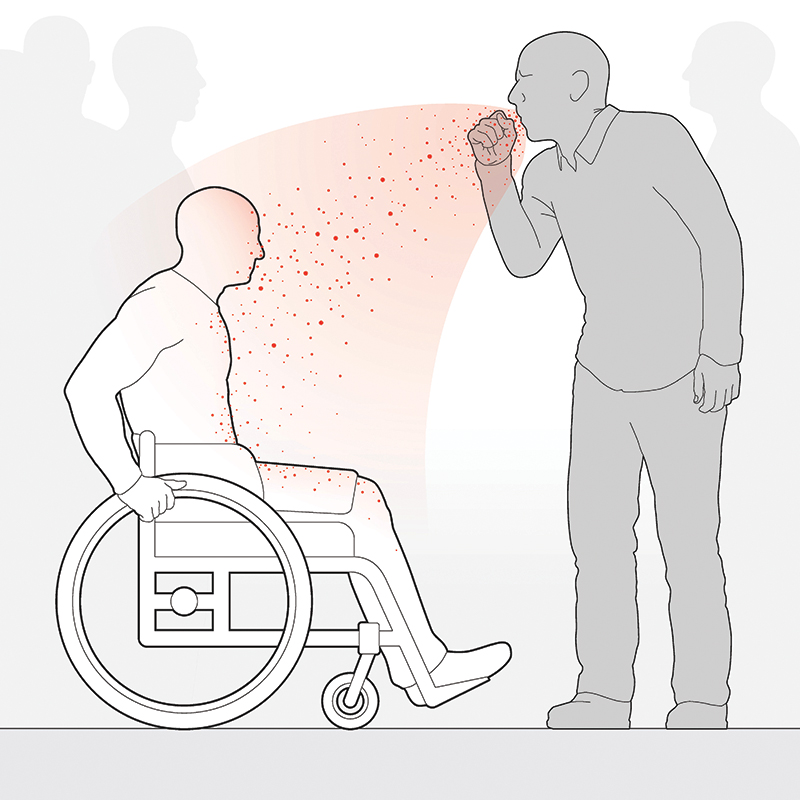
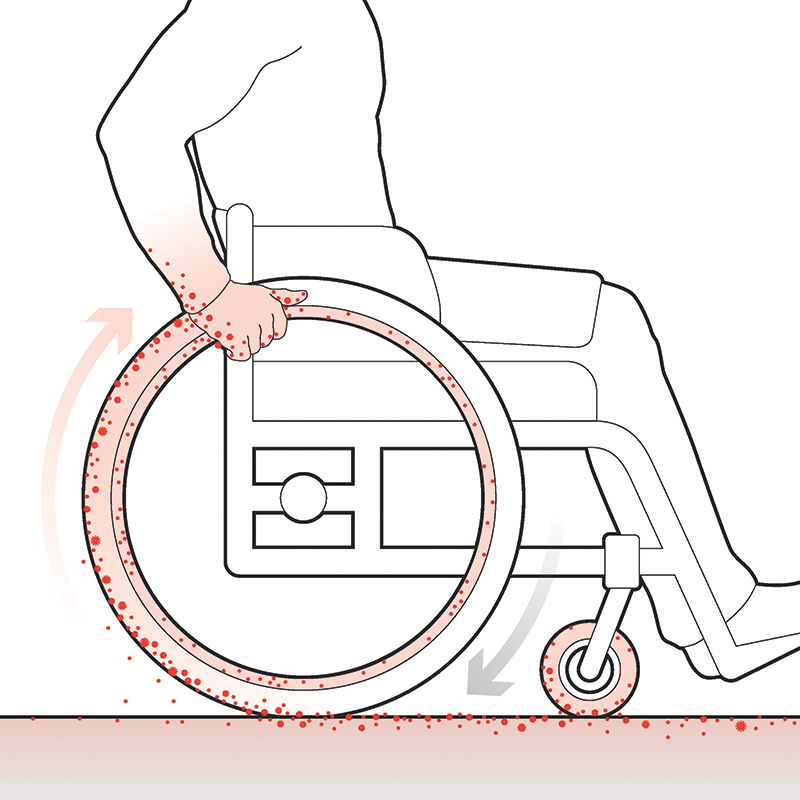
Because CoV-2 (and other) particles are heavier than air and because they sit lower than standing persons, a chair user is more easily infected. Additional factors contribute to potential contamination of the person, wheels, chair surfaces, controls, vehicles, and homes of chair users. For example, a study from a hospital in Guangzhou, China, found that 50 percent of the soles of the shoes of the staff contained traces of the CoV-2 virus. Floor contamination has not been addressed in any substantive way.
In the panic cycle of 2020, businesses rushed to install temporary plexiglass barriers with openings for payments and communication. The height of those openings establishes a direct line between the standing person and a chair user, creating unintentional discrimination that also affects people with hearing impairments, since talking through barriers is difficult even for persons with normal hearing and without masks. To effectively address this disparity, a national standard for filtration and effective communication with intercoms and active/passive talk ports in security glazing is needed.
Touching, Time, and Exposure
The earlier testimonies of people with vision impairments underscore the realities of interacting with a facility by touch. For persons with blindness or other visual infirmities, the need to navigate a space through touch — and the subsequent risk of pathogen transfer — is inherently increased. For the deaf-blind, there are even fewer architectural cues for wayfinding, locating elements, and reducing the amount of time in a structure.
Touching, time, and risk of pathogen exposure are positively correlated, meaning that the greater amount of time people spend inside a space and the more people they interact with and surfaces they touch, the greater their risk of exposure to pathogens. Factors that affect the duration of exposure for the vision- and hearing-impaired include effective signage with tactile characters and Braille, even in locations where they may not be required by regulations. Digital wayfinding and alarm notification systems that work with smart phone apps have accessibility features, and incorporating the use of a “Siri” or “Alexa” voice-command technology could be a strategy for locating the faucets, soap, and hand dryers.
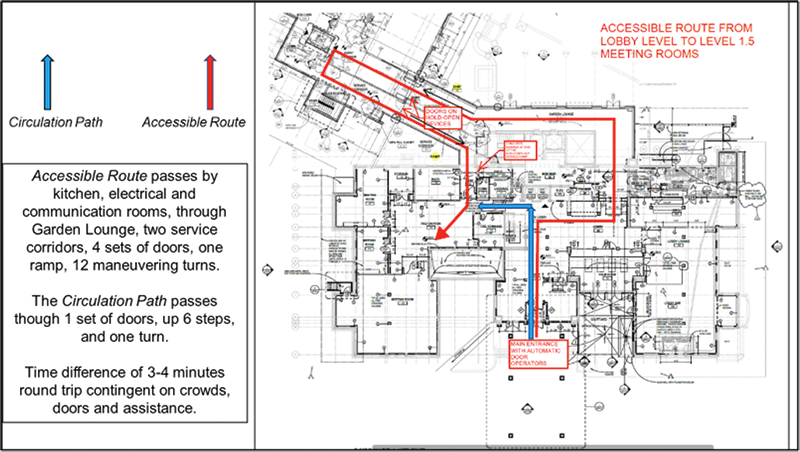
Additionally, ensuring that PWD can take the same circulation path of travel as the able-bodied is also critical in limiting duration of exposure. Both vertical and horizontal accessible routes should coincide with the circulation path for the able-bodied, meaning that entrances, stairs, elevators, lifts, escalators, and so on should be in the same space or area. No one should have to backtrack to find an accessible route or be separated from companions and caretakers to reach the same destination — and the less time that is spent in a facility, the less touching is required.
Technological Solutions
Today, there are technologies and advancements that, for the first time, present the design industry with tools to reduce the spread of diseases in buildings. Electricity — a relatively new technology when viewed in the history of pandemics — is pivotal, allowing for computerized HVAC controls for fresh air ratios, drones that can sanitize an entire arena, robotics to sterilize wheelchairs or whole buildings while empty, FAR UV-C lighting in return air plenums, numerous technologies within restrooms and hospital rooms, touchless door openers, touchless faucets, and touchless payment systems.
HVAC and Ultraviolet Lighting
In March 2020, Underwriter Labs approved the use of FAR UV-C lighting, which uses a specific wavelength of light to kill pathogens, for sterilizing large medical equipment. UV-C lighting and HVAC design are two emerging heroes. The introduction of UV-C lighting in return air plenums is a simple, cost-effective measure for sanitizing plenums and supply ducts.
Strategies for a “COVID kill zone” above human occupancy areas involve strategic placement of UV-C lighting and HVAC registers. The American Society of Heating, Refrigerating, and Air Conditioning Engineers (ASHRAE) and the American Society for Health Care Engineering (ASHE) are at the forefront of effective responses to pathogen control, and the 2019 ASHRAE Handbook provides multiple HVAC design strategies.
Fixtures and Filtration
Many touchless faucets utilize a reservoir to store water for instantaneous response. The water temperature and percentage of chlorination create potential conditions for breeding pathogens. ASHE reports that touchless faucet reservoirs can create a six- to seven-fold increase in retained pathogens. In response, many manufacturers have incorporated a “water age” automatic mechanism to flush the reservoir at specific intervals without demand. Throughout India, piracy and subsequent contamination of water supplies has been a problem as the population surges. In response, commercial and private water systems are using ultraviolet germicidal irradiation (UVGI) for small reservoirs, in-line instant water delivery, and other applications.
Many commercial hand dryer manufacturers have introduced gasketed filtration systems certified by the National Sanitation Foundation that entirely separate incoming and outgoing air with HEPA filters that trap particles down to .5 microns in size. As with other pro/con solutions, which will be discussed in more detail later, the intense decibel level of some hand-drying products can trigger autism spectrum or seizure disorders and exacerbate tinnitus and hyperacusis for the hearing impaired. A Quiet Mark Certification from the Noise Abatement Society is one consideration for the hearing impaired.
Materials
Other design factors that directly affect viral viability — how long a pathogen can survive — include material choices, particularly in finishing surfaces. Steel, plastics, cardboard, paper, copper, and wood all present different rates of viability. For example, inactivation of the SARS-CoV-2 on more porous surfaces is attributable to capillary action and faster droplet evaporation.
Pros and Cons
Open Floor Plans
It is important to note that some pandemic hardening strategies lower certain risks while increasing others, or benefit some groups of people while putting others at a disadvantage. For example, open floor plans with external fenestrations can provide quality views to the outdoors and bring in sunlight, which kills CoV-2 viruses in 7–8 minutes. Open plans also allow for better mobility and enhanced communication. But open or flex floorplans also enable a higher rate of pathogen spread. A two-year study study in Sweden involving open floor plan models with 1,852 participants found a “significant excess risk for sickness absence for short-term illness in three open floor plans” and “longer term illness for women.” Additionally, the reverberation rate and decibel levels of open plan spaces can increase tinnitus and hyperacusis for the hearing impaired. Promisingly, the ICC has developed new classroom acoustic standards that may be useful in open floor configurations.
Doors
Model codes rely on compartmentalization and doors for building classification, security, approach, entry and egress, privacy, fire and smoke spread, and so on. During design, zoning HVAC systems to control fresh air ratios, temperature, etc., to separate spaces is a simple solution. These systems in addition to positive/negative air pressure controls are essential in infectious disease wards.
However, disease spread, costs, injuries, and other factors are informed by the differences between installing a door or recognizing when they are unnecessary. A single commercial fire-rated door and appurtenances can easily cost $6,000. A privacy screen has fewer upfront and latent costs than a door, but pathogen spread may be increased. With privacy screens, people with vision impairment do not need to feel around for door openers or handles, etc., and chair users have an easier time navigating open door frames.
Anecdotal reporting indicates that the removal of doors — particularly in public toilet rooms — results in diminished door injuries and fatalities among the elderly and children. The presence or absence of doors also informs security demands and incidents, teacher interventions with students, firefighter rescue, and response times.
Moving Forward
The design community is, in general, made up of compassionate and caring people working toward equity, diversity, and inclusiveness. That commitment in response to this pandemic is obvious in the efforts of many groups and organizations — too many to list in this article. Knowing what questions to ask is as critical as finding the correct answers. The industry and individual practice of architecture are still learning how to do both well as the current pandemic, now in its third year, continues. As society moves past the panic and neglect cycles of this disease, a paradigm of pandemic hardening offers a more stable approach to controlling diseases than relying on human behaviors alone.
Richard Sternadori, MA. Arch., M. Ed., Assoc. AIA, is the senior program coordinator, researcher, and honorary faculty at the Great Plains ADA Center, University of Missouri, Department of Architectural Studies. He is a member of the TxA Equity, Diversity, and Inclusion Committee and the International Code Council Assisted Toileting and Bathing Committee.

Richard Sternadori, Assoc. AIA, M.A. ARCH, M. ED, CBO, CRC, ACTCP, retired in 2025 as the senior program coordinator, adjunct faculty, and research principal investigator with the University of Missouri Department of Architectural Studies, Great Plains ADA Center. He holds a Master of Arts/Architecture and a Master of Education in psychology with a focus on disability rehabilitation.